I did not see this video you posted. Thank you!Did you watch the full video of Campbell? Because he goes on to explain. The average age of death in the UK is 82.5. And most folks near that age have co-morbidities. So, it would be rare for someone that age to not have co-morbidities listed on the death certificate. It only points out something we know, Covid alone rarely kills healthy individuals, it is when it is combined with other disease processes that it hastens death.
The follow up video: after being critisized by the BBC.

Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
There are no long term adverse effects of mRNA vaccines
- Thread starter Dhersh
- Start date
- Status
- Not open for further replies.

This is a misnomer. We are moving into the endemic stage, which is very different than "making it history." We needed to pass through the acute stage and no matter of mitigation was going to avoid that. Thankfully, we found a very effective vaccination quickly, which allows us to eventually break the worst part of the virus, it's virulence, leading to hospitalizations and deaths at a high level. The overall cumulative hospitalization rate for those with Covid during their time of hospitalization is .9% or 913 out of 100,000. (Note this doesn't say that Covid caused their hospitalization). The current weekly rate is 8.9 out of 100,000 or .009%. In the endemic stage we should see that go down from there significantly. But, the important part to understand is that Covid isn't disappearing. It will still sicken, hospitalize and kill folks, mostly older folks despite vaccination status. (Average age of death is over 80).The minimal effort it takes to make this thing history seems to be too much for some people. I don’t celebrate that.
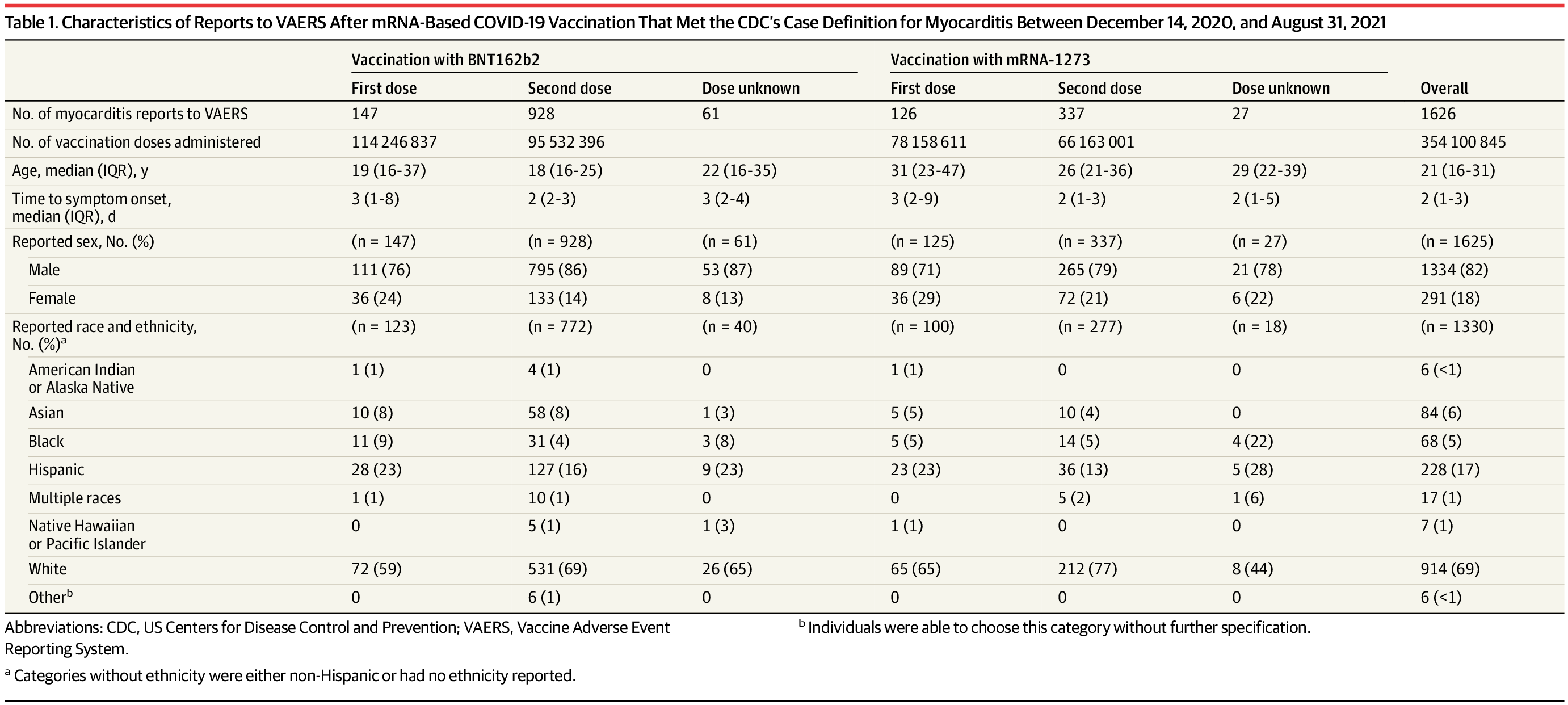
Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021
This descriptive study compares the effect of mRNA-based COVID-19 vaccination with BNT162b2 (Pfizer-BioNTech) vs mRNA-1273 (Moderna) on the reported cases of myocarditis in the US after each vaccination dose.
 jamanetwork.com
jamanetwork.com
Extremely small risk with no deaths and around 800 hospitalizations, mostly for observation.
Here is the relevant paragraphs from a study:
Among 192 405 448 persons receiving a total of 354 100 845 mRNA-based COVID-19 vaccines during the study period, there were 1991 reports of myocarditis to VAERS and 1626 of these reports met the case definition of myocarditis. Of those with myocarditis, the median age was 21 years (IQR, 16-31 years) and the median time to symptom onset was 2 days (IQR, 1-3 days). Males comprised 82% of the myocarditis cases for whom sex was reported. The crude reporting rates for cases of myocarditis within 7 days after COVID-19 vaccination exceeded the expected rates of myocarditis across multiple age and sex strata. The rates of myocarditis were highest after the second vaccination dose in adolescent males aged 12 to 15 years (70.7 per million doses of the BNT162b2 vaccine), in adolescent males aged 16 to 17 years (105.9 per million doses of the BNT162b2 vaccine), and in young men aged 18 to 24 years (52.4 and 56.3 per million doses of the BNT162b2 vaccine and the mRNA-1273 vaccine, respectively). There were 826 cases of myocarditis among those younger than 30 years of age who had detailed clinical information available; of these cases, 792 of 809 (98%) had elevated troponin levels, 569 of 794 (72%) had abnormal electrocardiogram results, and 223 of 312 (72%) had abnormal cardiac magnetic resonance imaging results. Approximately 96% of persons (784/813) were hospitalized and 87% (577/661) of these had resolution of presenting symptoms by hospital discharge. The most common treatment was nonsteroidal anti-inflammatory drugs (589/676; 87%).
Here is an comparison to viral derived myodarditis:
However, the onset of myocarditis symptoms after exposure to a potential immunological trigger was shorter for COVID-19 vaccine–associated cases of myocarditis than is typical for myocarditis cases diagnosed after a viral illness.24-26 Cases of myocarditis reported after COVID-19 vaccination were typically diagnosed within days of vaccination, whereas cases of typical viral myocarditis can often have indolent courses with symptoms sometimes present for weeks to months after a trigger if the cause is ever identified.1 The major presenting symptoms appeared to resolve faster in cases of myocarditis after COVID-19 vaccination than in typical viral cases of myocarditis. Even though almost all individuals with cases of myocarditis were hospitalized and clinically monitored, they typically experienced symptomatic recovery after receiving only pain management. In contrast, typical viral cases of myocarditis can have a more variable clinical course. For example, up to 6% of typical viral myocarditis cases in adolescents require a heart transplant or result in mortality.27
And finally:
The team determined the risk of myocarditis to be 0.146% among those with COVID-19 and 0.009% among those not diagnosed with COVID-19. During March 2020–January 2021, patients with COVID-19 had nearly 16 times the risk for myocarditis compared with patients who did not have COVID-19, and risk varied by sex and age.
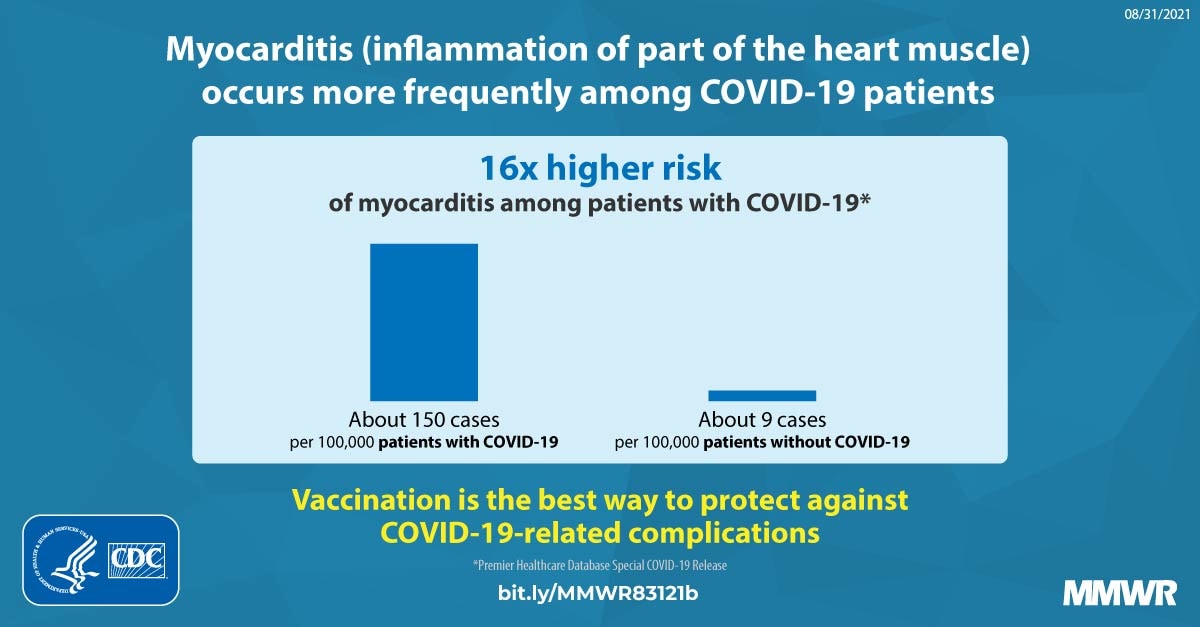
Association Between COVID-19 and Myocarditis...
Viral infections are a common cause of myocarditis. Some studies have indicated an association between COVID-19 and myocarditis.
 www.cdc.gov
www.cdc.gov
This has to be the dumbest post I have read. Thanks for the laugh. I actually feel bad for people so weak minded like yourself.If even half of the nearly 1MM reported to have died died because of Covid, that is more than the US lost in World War 2. What is even worse is that many of the people who died were people who survived that war. "Opinions" like yours are the problem. Sorry, not sorry. Your entire life is regulated by the government. There are laws against speeding, because it endangers other. You can't yell fire in the theater, because it endangers others. You are not free to assault people without consequences. Because it endangers others. You can't smoke on an airplane, because it endangers others. You can't drink and drive, because it endangers others. I don't give a F&*K if you don't want the vaccine. I really don't. But you shouldn't be allowed on a plane, in a restaurant, school or in a hospital, because . . . yep, you guessed it, it endangers others. Are the vaccines fully protective? As discussed elsehwere in this thread, nope. Almost no vaccine actually is. But that's no excuse. You are free to not get it. Just as you are free to shoot someone. But there are and should be, consequences for both.
800 reported hospitalization. Many go unreported, the reporting system need to be fixed to make report less time consuming.Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021
This descriptive study compares the effect of mRNA-based COVID-19 vaccination with BNT162b2 (Pfizer-BioNTech) vs mRNA-1273 (Moderna) on the reported cases of myocarditis in the US after each vaccination dose.
Extremely small risk with no deaths and around 800 hospitalizations, mostly for observation.
Here is the relevant paragraphs from a study:
Among 192 405 448 persons receiving a total of 354 100 845 mRNA-based COVID-19 vaccines during the study period, there were 1991 reports of myocarditis to VAERS and 1626 of these reports met the case definition of myocarditis. Of those with myocarditis, the median age was 21 years (IQR, 16-31 years) and the median time to symptom onset was 2 days (IQR, 1-3 days). Males comprised 82% of the myocarditis cases for whom sex was reported. The crude reporting rates for cases of myocarditis within 7 days after COVID-19 vaccination exceeded the expected rates of myocarditis across multiple age and sex strata. The rates of myocarditis were highest after the second vaccination dose in adolescent males aged 12 to 15 years (70.7 per million doses of the BNT162b2 vaccine), in adolescent males aged 16 to 17 years (105.9 per million doses of the BNT162b2 vaccine), and in young men aged 18 to 24 years (52.4 and 56.3 per million doses of the BNT162b2 vaccine and the mRNA-1273 vaccine, respectively). There were 826 cases of myocarditis among those younger than 30 years of age who had detailed clinical information available; of these cases, 792 of 809 (98%) had elevated troponin levels, 569 of 794 (72%) had abnormal electrocardiogram results, and 223 of 312 (72%) had abnormal cardiac magnetic resonance imaging results. Approximately 96% of persons (784/813) were hospitalized and 87% (577/661) of these had resolution of presenting symptoms by hospital discharge. The most common treatment was nonsteroidal anti-inflammatory drugs (589/676; 87%).
Here is an comparison to viral derived myodarditis:
However, the onset of myocarditis symptoms after exposure to a potential immunological trigger was shorter for COVID-19 vaccine–associated cases of myocarditis than is typical for myocarditis cases diagnosed after a viral illness.24-26 Cases of myocarditis reported after COVID-19 vaccination were typically diagnosed within days of vaccination, whereas cases of typical viral myocarditis can often have indolent courses with symptoms sometimes present for weeks to months after a trigger if the cause is ever identified.1 The major presenting symptoms appeared to resolve faster in cases of myocarditis after COVID-19 vaccination than in typical viral cases of myocarditis. Even though almost all individuals with cases of myocarditis were hospitalized and clinically monitored, they typically experienced symptomatic recovery after receiving only pain management. In contrast, typical viral cases of myocarditis can have a more variable clinical course. For example, up to 6% of typical viral myocarditis cases in adolescents require a heart transplant or result in mortality.27
And finally:
The team determined the risk of myocarditis to be 0.146% among those with COVID-19 and 0.009% among those not diagnosed with COVID-19. During March 2020–January 2021, patients with COVID-19 had nearly 16 times the risk for myocarditis compared with patients who did not have COVID-19, and risk varied by sex and age.
Association Between COVID-19 and Myocarditis...
Viral infections are a common cause of myocarditis. Some studies have indicated an association between COVID-19 and myocarditis.
- Status
- Not open for further replies.
Similar threads
- Replies
- 16
- Views
- 888
ADVERTISEMENT
Latest posts
-
-
 Softball FSU softball picks up another run-rule win vs. UNC
Softball FSU softball picks up another run-rule win vs. UNC- Latest: Seminoles70
-

-
-
ADVERTISEMENT